SpendRule Raises $2M to Help Hospitals Track and Control Spending
Product
The Law of Spend Entropy: Why Business Expenditure Decays Without Active Control
Written by

Joseph Akintolayo
Co-Founder
Date published
Reading time
Share blog

Business spend entropy is the natural tendency of organizational expenditure to drift toward inefficiency and misalignment without active management. This paper names the pattern, documents it in initial deployment findings, and makes the case for a contract-to-payment control architecture as the new standard of enterprise spend governance.
Key Findings
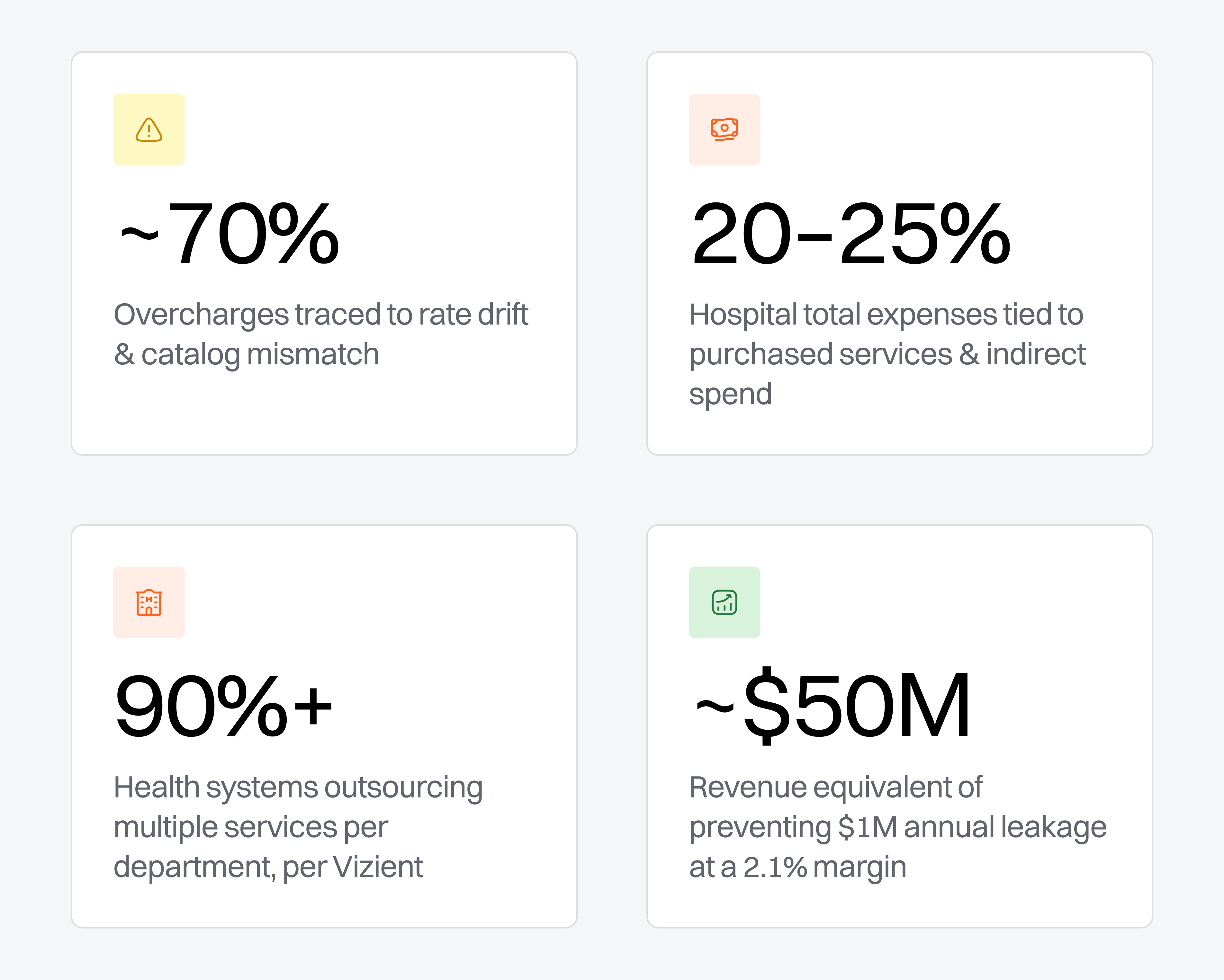
Leakage is structural, not accidental. Rate drift and catalog mismatch alone account for roughly 70% of verifiable overcharges, consistently, across vendor types and health system sizes.
The scale is enterprise-level. Purchased services, the largest undercontrolled cost category in healthcare, carry weaker invoice controls than any other major expense line.
Manual review has hit its ceiling. A large health system processes 200,000+ purchased services invoices per year, equivalent to 20+ full-time AP analysts just for validation.
The solution is architectural. A contract-to-payment control plane, not more headcount, is what turns negotiated terms into operational enforcement.
Prevention compounds; recovery does not. Every vendor in live monitoring becomes a permanent control. The economic case is ongoing margin recapture, not one-time savings.
Every Business Leader Understands Growth. Fewer Understand Decay
Growth is visible. It shows up in new revenue, new customers, more vendors, more contracts, more invoices, more complexity. Decay is quieter. It hides in rate schedules, amendments, vendor master records, and approval workflows. It does not usually look like a crisis. It looks like normal business.
In physics, entropy describes the tendency of a system to move from order to disorder without applied energy. The same law applies to business operations. Without active control, contracts drift from invoices, vendors drift from negotiated terms, and amendments drift from original agreements.
Health systems negotiate aggressively. But negotiated savings often never reach the P&L. In many organizations, vendor invoices are approved and paid without being validated against the actual terms of the contract. Over time, small discrepancies, such as incorrect rates, outdated catalogs, missed amendments, compound into material financial leakage.
We refer to this pattern as business spend entropy — the natural, inevitable tendency for organizational expenditures to become inefficient and misaligned over time.
Spend entropy's symptom is expense friction — the gap between what an organization should spend under contracted conditions, and what it actually pays because of vendor drift, missed terms, and operational waste.
Every unnecessary dollar spent means the organization must earn more just to offset what it should never have paid. In healthcare, where operating margins sit in the low single digits, that arithmetic is unforgiving.
Healthcare Is Entering the Entropy Era
The American Hospital Association reported hospital expenses grew 7.5% in 2025¹ — more than twice the growth rate of hospital prices. Kaufman Hall data shows margins have stabilized into a fragile "new normal," still pressured by payer mix deterioration and the structural gap between gross and net operating revenue.² Health systems are being forced to control leakage, not just grow revenue.
Contracts Are Not Enforced at Payment
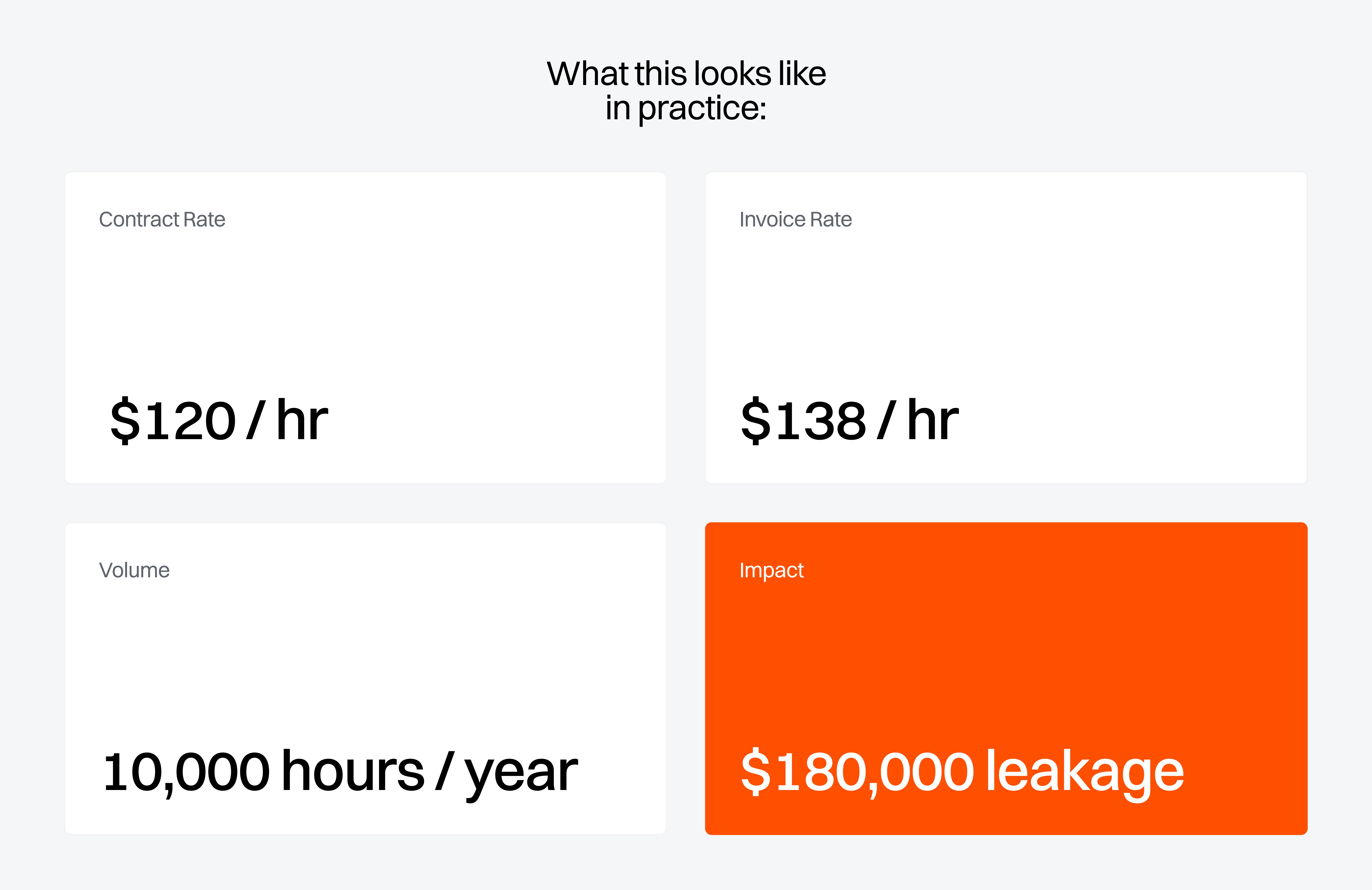
Most health systems are already negotiating. The problem is that negotiated terms often do not become operational controls. A health system may negotiate a better rate, but if the invoice is paid against the wrong rate, the savings never become real. A staffing agreement may define shift differentials, weekend rates, and location-specific pricing, but if nobody validates the invoice line against the contract, the wrong rate can keep flowing through AP indefinitely.
Most organizations have systems of record. Few have systems of enforcement. ERPs process payments. CLMs store contracts. AP systems route invoices. But between the contract and the invoice, there is often no active control layer. That gap, the contract-to-payment gap, is where entropy lives.
For finance leaders, the correct frame is payment integrity, not procurement compliance. The same discipline applied to duplicate payment detection and fraud controls should extend to rate validation on contracted services. When AP approves a purchased services invoice without checking it against the executed contract, that is an uncontrolled financial risk, not a sourcing oversight.
When You Look, You Find It. Every Time
In initial validation pilots across health systems, first-wave analysis of 5–10% of vendors consistently surfaced verified overcharges at the invoice line level. In every case, the pilot surfaced verified line-level overcharges with a projected annual prevention opportunity that scales substantially when extrapolated to the full vendor base.⁸ The leakage follows a consistent taxonomy:
Table 1 — Control Gap Categories Observed Across Purchased Services Deployments
Control Gap Type | Typical Share | What It Means |
|---|---|---|
Rate Drift | ~43% | Invoiced rate did not match contracted rate |
Catalog Mismatch | ~26% | Vendor catalog diverged from negotiated agreement |
Staffing Overage | ~22% | Hourly or shift rate exceeded agency contract terms |
License / Term Gap | ~5% | Software billed at list price instead of enterprise terms |
Other / Mixed | ~4% | Rounding, multi-site drift, miscellaneous issues |
Rate drift and catalog mismatch account for ~69% of overcharges, not as one-off errors but as recurring structural drift between what was contracted and what was billed. What makes this concrete is the invoice complexity involved: a single multi-facility services invoice with eight line items, different locations, prorated billing periods, amendment credits, takes a trained AP analyst 20–30 minutes to validate manually.
You Cannot Hire Your Way Out of This
The instinct is to add more AP oversight. But the volume has already exceeded what people can do. A large health system processes upward of 200,000 purchased services invoices per year at four or more lines each. Line-level validation at that scale would require 20+ dedicated full-time analysts, working exclusively on purchased services, year-round. No health system is hiring for that, and even if they did, the underlying data fragmentation would remain unsolved.

The Missing Layer: A Contract-to-Payment Control Plane
Purchased services have no SKU, no item master, no simple goods receipt, no standardized rate card. The proof of what was agreed lives inside contracts, amendments, exhibits, rate tables, location-specific terms, and free-text invoice descriptions. That makes them the ideal category for an AI-native control system: too nuanced for simple matching rules, too voluminous for human review.
This is not a procurement optimization problem. It is a systems architecture problem — and it requires a systems architecture solution.
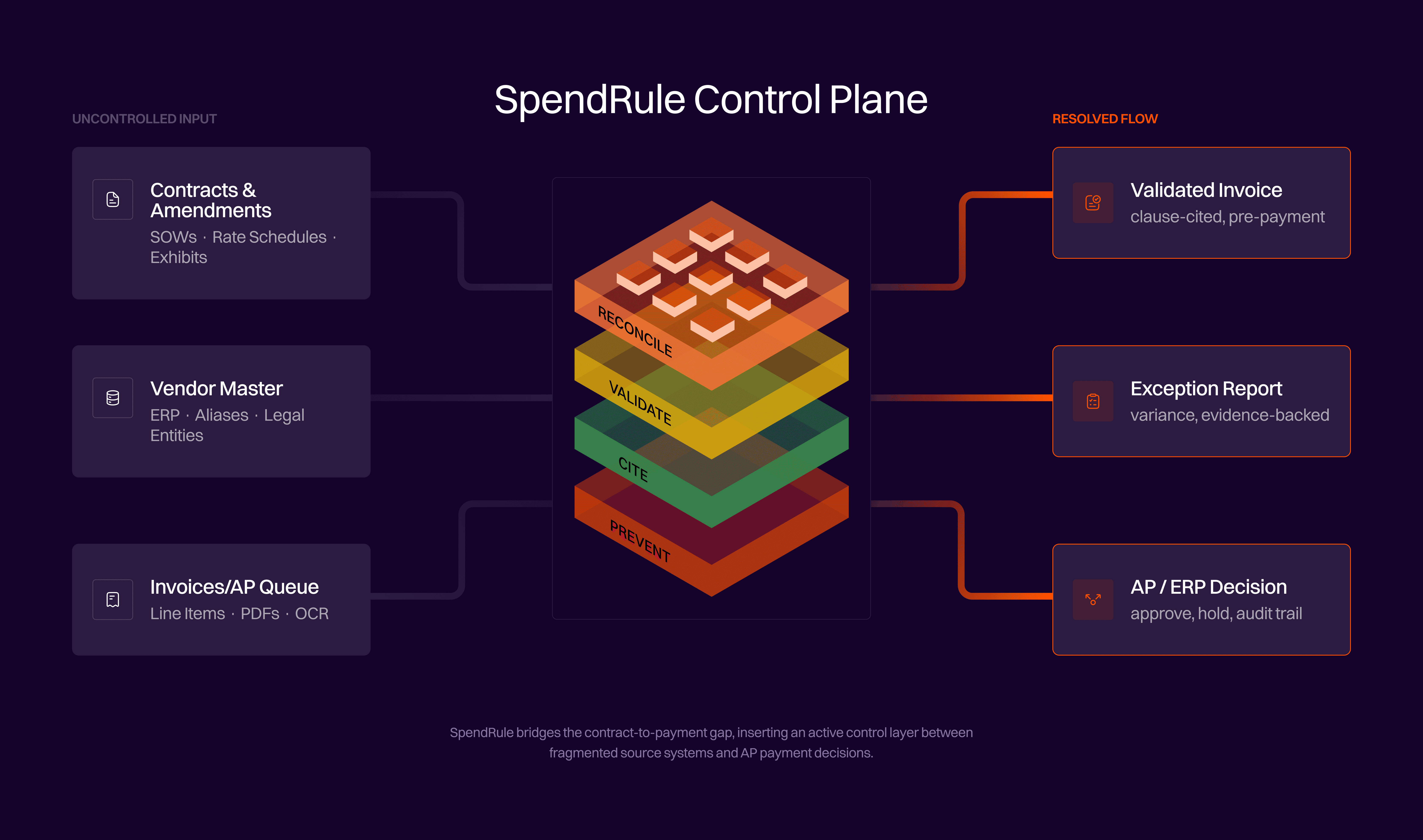
To address this, organizations require a contract-to-payment control architecture that connects contracts, invoices, vendor master data, and payment approval. That layer must:
Reconcile vendor identity across contracts, ERPs, AP systems, and vendor master records.
Parse service contracts, rate schedules, exhibits, and amendments into structured logic.
Match invoice lines to the correct contract terms and calculate expected charges.
Detect variance before payment approval.
Cite the exact source clause and page behind every finding, producing an evidence-backed exception AP, finance, and vendors can act on.
This is what turns a contract from a static document into an active financial control. SpendRule operationalizes this model within healthcare purchased services, where contract complexity, invoice variability, and vendor fragmentation make traditional controls ineffective.
From Retrospective Recovery to Front-End Prevention
The audit model assumes the damage is already done. A retrospective audit finds leakage after the money is gone. Recovery takes months, can become adversarial, and while the organization is recovering yesterday's leakage, the same control gap is producing tomorrow's. SpendRule is built on a different premise: prevent before pay.
Table 2 — Invoice Validation Maturity Curve
Stage | Timing | Value Delivered |
|---|---|---|
Traditional Audit | Months after payment | Retrospective recovery |
Pilot Validation | In AP queue or post-payment | Quantify and prove the gap |
Live Monitoring | Before payment approval | Prevent future overpayments |
Prevention is the better model economically. Retrospective audits recover approximately 14 cents per dollar of overcharge identified, after audit fees, vendor dispute cycles, and aged-payable write-offs. Prevention costs less than 5 cents per dollar. Every vendor brought into live monitoring becomes a permanent ongoing control.
Four Forces Making This the Right Moment
Fragile Margins. Costs outpaced prices by more than two to one in 2025. The margin compression is structural, not a temporary distortion that will self-correct.
Purchased Services Scale. Purchased services are large enough as a share of total hospital expenses to move the margin needle when brought under control. They are not a rounding error.
Structural Fragmentation. The outsourcing model has created contract complexity that manual AP was never built to govern. The gap between what was signed and what is billed compounds with every vendor added.
AI at Operational Scale. AI can now read contracts, interpret rate logic, reconcile invoice lines, and support continuous monitoring at enterprise scale. This was not viable before.
Expense Friction Becomes Revenue Friction
A dollar of preventable expense is not the same as a dollar of revenue. At a 2.1% operating margin, a single million dollars of preventable annual leakage represents a gross revenue equivalent of roughly $50 million, revenue the organization must generate harder just to absorb waste it should never have incurred. For a CFO, that is invisible margin pressure. For a supply chain leader, it is negotiated savings that never appear in operating results.
The critical distinction for finance is between random and systematic variance. Random variance self-corrects, errors in both directions net to zero over time. Rate drift is systematic: when a vendor invoices at an incorrect rate, that rate persists on every subsequent invoice until caught. FP&A teams running budget variance analysis are reading billed amounts, not agreed amounts, carrying an upward bias equal to the rate-drift margin, every period, every close.
Spend entropy is not a back-office problem. It is an enterprise performance problem.
Joseph Akintolayo,
CTO & Co-founder, SpendRule
Spend Control Is a Data Architecture Problem
Entropy exists because critical data lives in disconnected systems with no enforcing layer between them. Contracts live in CLMs. Invoices sit in AP queues. Vendor identity is fragmented across ERP records and aliases. Each system is doing its job. None is enforcing compliance at payment.
What health systems have today | What the architecture requires |
|---|---|
CLM — stores contracts, does not enforce them | Vendor identity resolution across all systems |
ERP — processes payments, no contract validation | Contract parsing — structured rate logic from document |
Procurement — approves spend, lacks invoice context | Amendment tracking applied at invoice time, not archived |
Retrospective audit — finds leakage months later | Rate computation from contract logic, not line matching |
Pre-payment exception — clause-cited, before cash leaves |
The enterprise does not have one spend truth, it has fragments. The technical challenge is turning those fragments into an enforceable knowledge graph and applying it at payment time. Resolving vendor identity alone, reconciling the name on an invoice against the name in a contract against the ERP record, can require processing tens of thousands of vendor master records. That foundational work is unglamorous, but it is where spend control is either built or broken.
Active Enforcement is the New Standard
The law is simple: spend left unmanaged will decay into leakage. Not because people are careless, but because complex systems drift. The contract says one thing. The invoice says another. The AP workflow optimizes for throughput, not compliance. That is entropy, and entropy always wins unless energy is applied.
The new standard for health systems is active spend enforcement: validating every eligible invoice line against the actual contract before payment approval. This level of enforcement requires more than incremental process improvement, it requires a system designed to connect contracts, invoices, and payment decisions in real time. SpendRule was built to deliver this capability for healthcare purchased services, where contract complexity and invoice variability have historically made enforcement impractical.
The question is no longer whether purchased services leakage exists. Deployment data proves it does. The question is whether the organization finds it after payment or prevents it before cash leaves. In a low-margin industry, entropy is not just disorder. It is lost margin. It is lost strategic flexibility. And in healthcare, it is lost resources that should have gone back into patient care.
See what spend entropy looks like in your vendor base.
Give SpendRule 10 contracts and 10 invoices. We analyze them to show you real savings opportunities, all in under 10 minutes.
Visit spendrule.com/10-10-10
References
American Hospital Association. "Report: Hospitals face increased challenges and financial pressures as they care for patients." March 2026. aha.org
Kaufman Hall. "National Hospital Flash Report: December 2025 Data." kaufmanhall.com
Kaufman Hall. "2025 Health System Performance Outlook: Redefining Resilience." December 2025. kaufmanhall.com (PDF)
Vizient. "Purchased Services for Healthcare Facilities." vizientinc.com
Premier, Inc. "Report: The Top 5 Areas of Purchased Services Spend and How Providers Can Improve Margin." premierinc.com
SpendRule internal deployment data.
SpendMend. "The Essential Role of Recovery Audits in Healthcare." spendmend.com
Joseph Akintolayo
Co-Founder
Share blog